

Recently, I read an article on surviving an edged weapon attack, where the writer spoke specific to knife wounds, as they related to unconsciousness and death, which I found quite troublesome given the fact that his numbers just did not reflect the empirical experience/data that I have witnessed over my 29yrs of being a law enforcement professional.
In this article, the author first quoted a book written by Captain W E Fairburn called “Get Tough: How to Win In Hand-to-Hand Fighting” published in 1942. On page 99 of this text (fig.112) Fairburn provides the following information specific to “loss of consciousness in seconds” and “Death” specific to knife wounds:
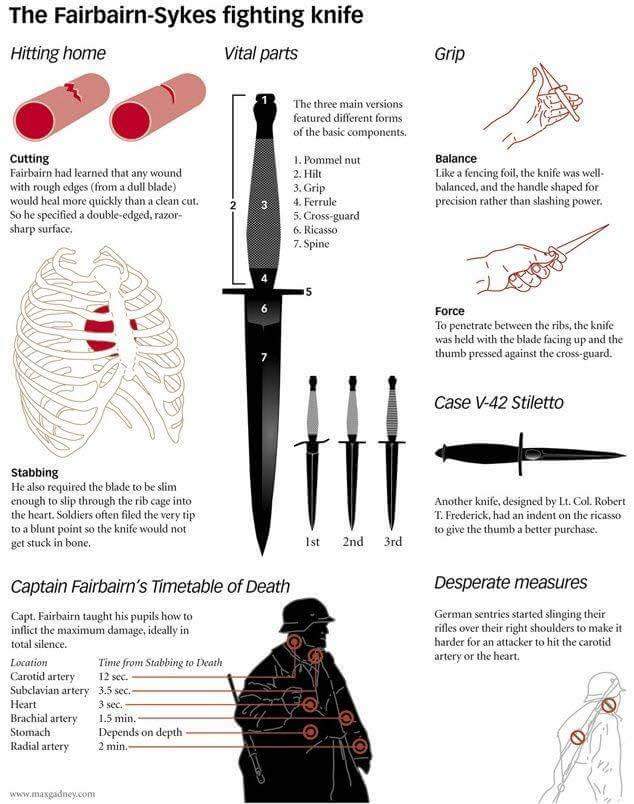
Brachial Artery – Unconsciousness 14 seconds, death 1.5 minutes
Radial Artery – Unconsciousness 30 seconds, death 2 minutes
Carotid Artery – Unconsciousness 5 seconds, death 12 seconds
Subclavian Artery – Unconsciousness 2 seconds, death 3.5 seconds
Heart – Unconsciousness instantaneous, death 3 seconds
Background
I attempted to locate any medical literature surrounding the time that this book was published to support the above noted data, but I was unable to do so. If anyone reading this can provide me with the medical literature that supports Fairburn’s data from that time period, please send it my way.
Based upon the above noted Fairburn data, I began my literary review of the martial art/self-protection/combatives academia, specific to unconsciousness and death specific to knife wounds, and what I found was very surprising if not troublesome. Much of the data supplied in these books, articles, and papers that I reviewed were just a rehash of Fairburn’s numbers, and others were anecdotal at best, and more often than not just plain negligent. None, and I mean none, cited any medical literature to support their claims. Some stated that they had spoken to a medical professional (doctors and paramedics) to validate their claims, but yet they did not provide the names of these medical professionals, or their credentials, or even medical research links which would have helped validate their published writings.
Research
After reading the above noted martial art, self protection, and combatives academia, and being less than impressed with their reported data specific to unconsciousness and death as it relates to knife wounds, I too decided to connect with the medical professionals. Two of the doctors that I connected with are experts in their field of medicine; both specialize in trauma care and critical care medicine, and have a plethora of firsthand experience in dealing with those who have been injured via an edged or pointed weapon:
Dr Lorne David Porayko:
• Full time Critical Care Medicine/Anaesthesiology specialist in Victoria, Vancouver Island Health Authority
• Critical Care team leader
• Works in conjunction with Dr Christine Hall
• Martial Arts background in Judo (black belt level), MMA, Krav Maga
• Honoured to say that Dr Porayko is one of my full time students
Dr Christine Hall:
• Full time emergency medicine specialist in Victoria, Vancouver Island Health Authority.
• Trauma team leader and educator.
• Previously, program director for emergency medicine at the University of Calgary.
• Master’s degree in epidemiology from the University of Calgary.
• Cross-appointed in the department of community health sciences through the faculty of medicine at the University of Calgary and also the faculty of medicine’s department of surgery at UBC.
Shock
When it comes to unconsciousness or death attributed to an edged weapon attack, we are talking about what the medical community calls “Shock”. Dr Porayko defines shock as, “the development of multi-organ failure due to insufficient oxygen being delivered to the tissue to meet their metabolic needs.”
Specific to shock as it relates to unconsciousness and death, Dr Porayko stated the following to me:
“ A 70kgs (154lbs) male’s circulating blood volume is about 70ml/kg which equals about 5 litres. Cardiac output is about 5-7 litres per minute. All the great vessels of the body act as a conduit of approximately 15-20% of CO/minute which equals about 1 litre per minute. The great vessels include the innominate artery, Subclavian arteries, carotid arteries and some include the iliac arteries. The 4 atria, 2 ventricles and aorta all conduct the full cardiac output thus are well protected in the centre of the body behind the sternum and in front of the thoracolumbar spine.”
So why is the above noted information important, because hemorrhagic shock (blood loss) is based upon how much hydraulic fluid (blood) is leaked from the body. When it comes to understanding hemorrhagic shock, I would guide you to the following links that were provided to me by Dr Porayko:
http://ccforum.com/content/8/
http://ccforum.com/content/8/
Dr Porayko advised that based upon the above noted link:
• A class II shock category (750-1500ml) would leave “most” dizzy and very weak
• a Class III or Class IV shock category (1500ml-2 litres of blood loss) would leave “most” with the inability to stand up right
Specific to my questions about unconsciousness and death if specific anatomical arteries or veins were cut, and given all the medical variable associated, the Doctors had to make the following assumptions first before they could answer my questions:
1. There is no compression of a lacerated artery underway. This was irrelevant for a lacerated vein due to the fact that a vein can’t be compressed
2. The subject is previously healthy with a normal haemoglobin concentration and has a normal VO2 max prior to being wounded.
3. If an artery is the target, the artery is incompletely transacted. Completely transacted arteries go into vasospasm and retract into their perivascular sheaths which markedly reduces bleeding and even stopping bleeding all together in the case of smaller vessels. On this point Dr Porayko stated that this is the reason the Ghurkhas were trained to twist their knives in the femoral artery after puncturing it- to avoid a clean surgical transaction, thus preventing the vasospasm and retraction into the perivascular sheath, and instead to intentionally cause a hole in the vessel sidewall which is much more lethal.
4. The adventitia (a saran wrap like layer around the blood vessel) does not seal the wound ( The doctors stated that this usually does happen in survivors) and/or a clot does no form after blood pressure drops.
The doctors also noted:
“although exsanguinations (death from blood loss) from a venous injury is much slower that an arterial one (because mean arterial pressure is usually at least 10x central venous pressure), the venous injury is much more difficult to treat and generally if arterial injured patients survive to hospital with manual compression, they will do well whereas major venous injured patients often die even after getting to the operating room”
Of note, both doctors opinioned that the numbers provided by Fairburn and other combative/martial arts instructors that I provided to them for review, specific to times for unconsciousness and/or death, are way too short. Both stated that they believed that these numbers are based upon “complete cessation” of all cardiac output through the involved vessel which is not the norm. In fact Dr Pryayko brought to my attention that during the French revolution when thousands of people were beheaded by guillotine, the attending doctors documented the presence of vital signs in the body for up to two minutes.
Real Numbers
So based upon the above 4 “assumptions”, here are the numbers that the doctors I consulted provided specific to a level of hemorrhagic shock taking place which would lead to unconsciousness or death in “most” situations:
Carotid Artery – Approx 2-20 minutes
Jugular Vein – Approx 15-60 minutes
Subclavian Artery – Approx 2-20 minutes. The doctors also noted: “this is a special circumstance anatomically because this vessel is protected by the clavicle and the first rib (sandwiched between them) if the Subclavian artery bleeds, the only way to compress it and repair it is to open the chest by thoracotomy. You cannot compress it. Patients usually die on the scene or en-route to hospital.
Subclavian Vein – Approx 15-60 minutes
Brachial Artery – 5-60 minutes. The doctors also noted: “pretty unusual to see these without compression by EMS)
Femoral Artery – 5-60 minutes. The doctors also noted: “Pretty unusual to see these without compression by EMS)
Aorta or any part of the heart – Approx 1-2 minutes. The doctors stated that the heart conducts 100% of cardiac output. Assuming transaction and that the hole does not seal. Ventricular holes do usually seal while the atrial ones do not due to the orientation of the muscle fibres.
Two other areas of note made by the doctors also included:
Popliteal Artery – Located behind the knee, would be similar (but slightly less) to cutting the femoral artery
Inferior Vena Cava – Can be attacked via a deep abdominal stab, similar to cutting the Jugular vein
Exceptions
Both doctors stated that these are estimates based upon current medical literature and their first hand experience, but both also stated that there are always exceptions to these estimates. Both gave examples where patients who had received severe knife wound survived even with a heavy loss of blood, some examples:
• One of the doctors has seen several patients with traumatic cardiotomies (a big hole in the heart) survive for 20 minutes before being treated
• One of the doctors treated a patient who had been stabbed in the abdomen, where the knife hit the inferior vena cava, his belly was full of blood, he was conscious, although shocky, an hour after the injury when he arrived in the ER. He survived.
The doctors stated that they have seen patients who have bled out nearly their entire blood volume, but yet are still awake and talking (although looking bad) many many minutes following an injury and survive to tell their story. Dr Porayko stated, “So it is a mistake to underestimate a person’s capacity to compensate for acute hypovolemia and anaemia (hemorrhagic shock), even when very severe. This is especially true in the younger population.
Conclusion
So why did I write this article?
1. Much of the information being propagated in the martial arts, self protection, and combatives industry specific to unconsciousness and death as a result of a knife attack, specific to blood loss, is inaccurate. I wanted to provide those who are looking to share current and accurate medical opinion with the above noted information, hoping that it will go viral in our industry. For those who don’t and continue to teach inaccurate information, shame on you.
2. Those who teach others how to fight with a knife, and state that if you cut or stab a person here or there an attacker will die in seconds, are both willfully blind and being irresponsible to their student in most cases. Those who teach others how to fight with a knife need to absorb the information in this article, and start teaching from a medically researched knowledge base.
The most important reason for this article, SURVIVAL !!!!!! Words are powerful, and can create our own reality. If you “believe” that you will die in seconds because your radial artery has been cut in a knife attack, and your instructor told you (and you believe him) that you only have 30 seconds to live before you die from blood loss, then you likely will die. As can be seen from the numbers provided by the doctors, even if one receives a severe cut or stab to a major blood vessel or organ, you can still fight for several minutes (not seconds), and even longer, and still survive. As Dr Hall stated, “The decision to survive, it is that intangible thing that cannot be measured, and I think is part of the reason that some people survive and some don’t. You have to decide ahead of time that you are going to live.”
————————————————————–
Darren Laur, also known as “The White Hatter”, has dedicated his life to public safety, and is a recently retired and highly respected Staff Sergeant with the Victoria City Police Department with over 29 years of law enforcement experience, and is a Certified Advanced Open Source Intelligence / Social Media Investigator with a strong interest/background in on-line and social media investigations. Darren is an internationally court recognized safety and workplace violence prevention expert/advocate, award winning published author and highly sought after international keynote speaker, who specializes in the area of personal safety and self protection both on-line and off-line.
More information can be found at: http://www.personalprotectionsystems.ca/






18 Responses
Also added should be the ‘gun vs knife’ debate. A lot of people believe that if they are carrying a firearm that they will have the upper room. I encourage anyone to Google and search the “21 foot rule”.
Here’s a good one too.
http://www.usadojo.com/articles/21-feet-valid.htm
Thank you for the excellent article. The people who taught me said they wanted to stop the fight. As a result they taught us to cut large tendons and muscles. If they can’t move it, they can’t use. Your article indicates why a severed tendon or muscle might be far more effective in stopping an assailant, than a slash to the carotid.
Yep… having seen someone stabbed several times… They dont even stop fighting. Watched a little guy stab this big biker 3 times before the biker got ahold of him and smashed the little guy against the nearest light pole.
One hit of the guys head against a metal pole and he was down. The big guy did not even drop to a knee until he walked about 50 feet away back towards the door.
i worked in a emergency room of a major northeastern metropolitan area hospital in the 70’s, a real knife and gun club area.
I saw many gsw and knife wounds, and the fatalities were considerably higher in the knife wound group. One teenager came in with a steak knife into his heart, the handle moving with every beat. Fortunately no one attempted to remove it or he would have been a goner. They oversewed the hole in the OR, taking it out under direct observation. He went home in 5 days. A less fortunate individual came in with a stab wound to the chest. We started an IV, was getting him ready for chest tube placement, he got up, tore out his IV, and stated he was going out to get that m….f….ker, and left. He came back 3 hours later, DOA, shot 4 times. Just thought i’d share the stories of mayhem and survival.
The US Army has done a great deal of research in regards to this subject based on lessons learned In the latest conflicts. This Information is pretty readily available, and, confirms what the writer is saying.
Seems to me that if one finds oneself in the vicinity of a person or persons waving a knife or gun about then one should look for an exit. Chances are any stab wound or bullet wound , if left unattended by a medical expert in these matters, , will succumb to the wounds . One minute or five minutes or fifty five minutes seems unimportant if the destination is the morgue.
Most of us have the capacity to recognize evil people , Darwin at work, and should be astute enough to get away as quickly and unobtrusively as possible.
The few police officers I have met seem as puzzled by violence as the rest of us. They just see more of it than most of us do so maybe stay calm in its midst.
I was thinking about this from the point of view of home defense. If one doesn’t have or is unable to get to ones gun in time it seems it would be better to have a baseball bat rather than a knife, For one you need to get pretty close to someone to use a knife, which exposes you to whatever weapon the intruder has. And second, as the author points out, even if you stab him he can still fight you for a while.
Michael Janich’s Contempory Knife Targeting: Modern Science vs W.E. Fairbairn’s Timetable of Death covers this subject extensively.
Glad to see people that do their homework. Even more impress they are fellow canadian, and doctor I have work with. Great article. It is time to fight the misinformation that has plague many survival website and youtube channel.
A fascinating post.
“…The most important reason for this article, SURVIVAL !!!!!! Words are powerful, and can create our own reality. If you “believe” that you will die in seconds because your radial artery has been cut in a knife attack, and your instructor told you (and you believe him) that you only have 30 seconds to live before you die from blood loss, then you likely will die…”
I have seen videos of police officers training in room clearance, where an officer gets shot with a paintball or Simunition and falls down. Why? Because after having seen it on TV for their entire lives, they have been conditioned to believe that that’s what happens.
Strive to emulate Master Sergenat Roy Benadidez.
Hello and you’ve effectively shown how books can not always contain true information and lead readers to believe falsities, much like television creates false beliefs in how things “should” happen. I’ve always relied on real life scenarios, real experienced people and only a couple books, with one recommendation. On Killing by Ret Col David Grossman shows how human animals improperly trained to fight for real, will do everything they can to avoid a fight. Two real life examples, 1986 FBI Miami shootout where an agent fired a fatal round into Platt(bad guy), yet Platt still fought, killing two other agents and seriously wounding another. http://lawofficer.com/2014/02/lessons-by-the-decades-the-fbi-miami-shootout/ And Trooper Coates was shot in his vest after a traffic stop, then hit his suspect 5 times in the chest with his .357. The suspect went down and while the trooper was able to get up, he exposed his side and under his armpit, where his vest didn’t cover. The suspect fired one .22 round into that arm hole. The round went through the troopers heart and he bled out there. The bad guy lived and was convicted of killing the trooper. http://www.odmp.org/officer/420-trooper-mark-hunter-coates Video here. http://youtu.be/2FraE77l4fI
And this is me on LinkedIn. It’s not my official resume but an wxplanation of my experiences just below my raceboat and name. . https://www.linkedin.com/m/profile/ACoAAAMmQQUBb4JF1gbcicOncL7X5W7lrDnUkJg/
I referenced gun fights here but my point is if you are going to research, look for reality, not book crap and train hard. Practice does not make perfect…Perfect practice makes perfect.
So a lesson here is… large knifes have a specific advantage, penetration. I am butcher/meat cutter with two decades plus experience and one thing I can tell you is every knife has a purpose. The second is anatomy, knowing where to cut. While working in a slaughterhouse we used “Hot Knifes” hollow ground, Never to hit a bone. While working as a breaker we used mostly an 8in or 10in curved breaking knife and semi flexible boning knife 6in.
As a collector of knifes I have too many, boxes upon boxes downstairs and maybe 200 upstairs, my nicer ones.
Having never been involved in a knife fight, I can’t tell anyone what’s best, but I think I’d want to have my Cold Steal carbon blade bowie. That said I do have about 15 or 20 stilettos of various lengths.
I have seen a very intense very short melee between two healthy males, one armed with a knife and one armed with only his fists. I can tell you all for a fact that the unarmed guy never even felt the knife wounds to his body and was not aware he was being stabbed. He beat the knife wielder unconscious and then walked away totally unaware that his intestines were hanging out and his pants and shirt completely soaked in his own blood. The knife had ZERO effect on his ability to fight.
Have you actually researched LtCol Wm E Fairbairn? If not then you should. While the good colonel may not have an MD, he does have a degree in BA (badass). Colonel Fairbairn was the foremost professional in hand to hand KNIFE combat (at the time and as far as I know to date) and had the bona fides for that title. I won’t bore you with the obvious details that can easily be researched. Doctors give times associated with EMS care and the immediacy of attempted survival first aid…which has NOTHING to do with real world survival during life and death combat situations. When a fight ensues after a mortal (though not fatal) knife wound and your heart rate doubles or triples and your body is working at 100% output, I would suggest that whatever Fairbairn said was true. While I did not know him personally, I knew men (of honor) that had known him (them) and respected their high opinions of them. Fairbairn and his partner Eric Sykes taught American, English and Canadian commandos in WWII (and a small contingent of Poles). They also taught many of the Rangers that landed on D-Day. If the good colonel says that’s what happens, then by and large, THAT IS WHAT HAPPENS. He was not an armchair/internet commando with 29 years on a modern PD. And regardless of whom you contacted, he was a badass and had the scars to prove it after 20 years on the Shanghai Municipal Police department in the early 1900s. He fought in hundreds of hand to hand knife fights, DOCUMENTED AND WITNESSED, on Shanghai’s waterfront. I can’t think of a single person that I know of or have heard of that has the combat resume he has. I spent 38 years in the military, both active and reserve, in special units and assigned to “other government agencies” and as a “contractor” way before that was a “thang” and have had a lot of contact with similar people. And while all were badasses in their own right, none have the resume he has. It would be interesting to know how many “hand to hand” knife fights the OP has actually been in or seen. Most police departments don’t get in knife fights, ever, hence the reason for the handgun. I’m not sure that being in Victoria BC and on the PD qualifies one to comment on the “art of knife fighting” and the attendant results. Victoria, BC isn’t exactly the crime capital of North America, try Victoria Texas instead. LtCol Fairbairn is NOT a martial artist (though he was an expert in the martial arts) in the modern concept of the term. He was a badass and could back it up…and did many times over. To say that a wound, perpetrated in the absence of any other context, will be this or that, as the OP suggest is futile and facil. I would also agree with the OP that those that teach knife fighting “martial arts” are probably teaching ineffective skills. Fairbairn and Sykes used REAL KNIVES to teach knife fighting….!!! However, to attempt to diminish Fairbairn AND Sykes expertise, honor, and testimonies is less than well thought out and borders on dishonorable slander. I would go with their thoughts before going with the OP. Be Well.
TripodXL…. how many times does one need to say “badass” to try to prove a point? Point missed… you worship men unduly.
Mr.Laur,
Thank you for taking your personal time to research this information, and provide it to the readers of this blog. Having the ability to interact with medical professionals provides clarity to an area that is somewhat shrouded in mystique.
Information is just that information, it could be good or it could be misleading. The reader in turn will attempt to decipher that knowledge, until something else comes along to refute it or substantiate it.
I agree on the responsibility to teach correctly, however most schools do not teach the true lethality of combat. (oh boy now I opened a can of worms there) The average John Q Citizen does not understand all the variables that come into play. From the body’s own reaction to life threatening conflict, because after all it’s “training” in a controlled environment. This training takes place 2 times a week maybe, and the period of instruction is confined to an hour or two.
No fear factor here, no accelerated breathing, no real contact. No blood, no slippery handle that gets tacky, no understanding of the psychological impact the other person,or you will have when the cut/slash is made. Most places train using a hammer or ice pick grip, but what about the guy who has no training and just swings wildly. Unpredictable and still a threat, but people would write him/her off as no risk.
So they learn what is taught, of a civilian nature. Krav Maga, and Systema would come close to it for military mind set training, but in the end the only real true teacher is costly and carries a heavy penalty for mistakes. I’ll close with this saying.
The difference between life and a classroom is simple;
In the classroom you are taught a lesson that prepares you for a test.
In life you are tested to teach you a lesson.
Post Script:
To those that do not understand my comments sorry my English is ok but not great. I feel his information provided by those affiliated to the medical field allow credence to the write up and I find it quite informative.